physical therapy documentation examples pdf
Understanding Physical Therapy Documentation
Effective physical therapy documentation is crucial for patient care, legal compliance, and reimbursement. Examples readily available online, often in PDF format, showcase various note structures and phrasing. These resources provide templates and examples for different settings, including outpatient, inpatient, and home health, offering guidance on documenting subjective, objective, assessment, and plan components. Proper documentation ensures accurate record-keeping and facilitates efficient communication amongst healthcare professionals, ultimately improving patient outcomes. Downloadable examples are invaluable for learning best practices.
Importance of Accurate Documentation
Precise and comprehensive physical therapy documentation is paramount for several critical reasons. First, it serves as a legal record of the patient’s treatment, protecting both the therapist and the patient. Thorough documentation supports the medical necessity of services, justifying billing practices and ensuring appropriate reimbursement. It also aids in tracking patient progress, allowing for timely adjustments to the treatment plan. Accurate documentation is essential for effective communication among healthcare professionals involved in the patient’s care, fostering collaborative decision-making. Furthermore, it forms the basis for evidence-based practice, contributing to the advancement of physical therapy knowledge. Without accurate documentation, the quality of patient care can be compromised, as well as the ability to demonstrate the value and effectiveness of physical therapy interventions. In essence, accurate documentation is the cornerstone of high-quality, accountable, and legally sound physical therapy practice. The readily available examples in PDF format serve as excellent tools for mastering this essential skill, ensuring that documentation is both comprehensive and compliant with professional standards.
Legal and Ethical Considerations
Physical therapy documentation is subject to stringent legal and ethical guidelines. Accuracy is paramount to avoid legal repercussions, ensuring that all entries reflect the actual services provided and patient interactions. Maintaining patient confidentiality is a critical ethical responsibility; all documentation must adhere to HIPAA regulations and relevant privacy laws. Falsifying records is unethical and illegal, carrying severe consequences. Furthermore, documentation must be objective, avoiding subjective opinions or biases that could jeopardize professional credibility. Therapists must ensure that their notes clearly demonstrate the medical necessity of their interventions, justifying the use of resources and the overall treatment plan. Adherence to professional standards of practice is vital, requiring a thorough understanding of appropriate documentation techniques and terminology. The use of readily available examples and templates, such as those found in PDF format online, can help physical therapists navigate these complex legal and ethical considerations, ensuring their documentation is both compliant and ethically sound, safeguarding both the patient and the practitioner. Regular review of professional guidelines and legal updates is essential for ongoing compliance.
Common Challenges in Documentation
Physical therapists often face several challenges in documenting patient care effectively. Time constraints are a significant factor, with many therapists reporting insufficient time to thoroughly document each session. The complexity of accurately reflecting the nuances of patient progress and response to treatment can also be difficult. Maintaining consistency in documentation style and terminology across different settings or healthcare systems presents additional hurdles. The sheer volume of information needing to be recorded can lead to feelings of overwhelm and potential errors. Difficulties in integrating electronic health record (EHR) systems into clinical workflow further complicate the process. Furthermore, ensuring that documentation accurately captures both the skilled nature of interventions and the medical necessity of services is crucial for reimbursement purposes but can prove challenging. Access to appropriate resources, including readily available examples and templates (such as downloadable PDFs), can mitigate some of these issues, streamlining the documentation process and improving the quality and consistency of records. Clear guidelines and standardized formats can improve efficiency and reduce the risk of errors or omissions.
Essential Components of PT Documentation
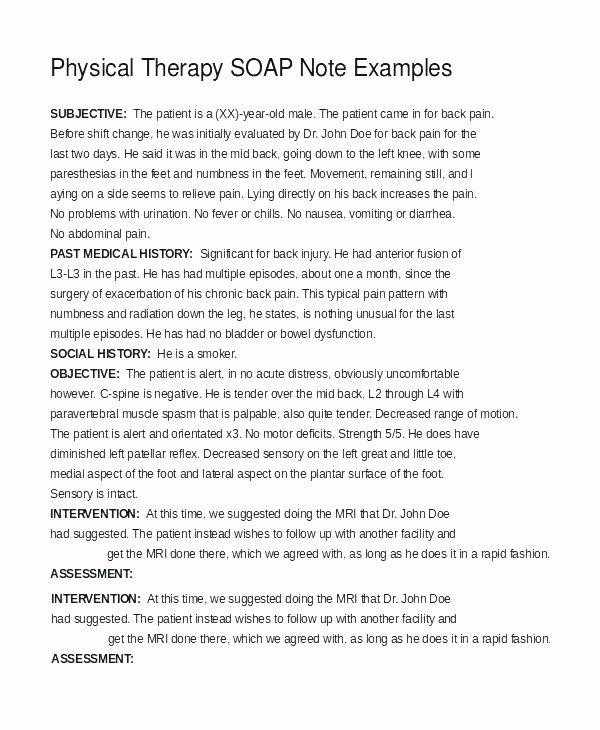
Comprehensive physical therapy documentation typically includes subjective and objective findings, assessment of the patient’s condition, a detailed treatment plan, and progress notes. These components, often structured using SOAP note format (Subjective, Objective, Assessment, Plan), are crucial for effective communication and care coordination. Examples in readily available PDFs demonstrate these essential elements.
Subjective (S)⁚ Patient Reported Information
The subjective section of a physical therapy SOAP note captures the patient’s self-reported experiences and perspectives. This crucial component relies heavily on the patient’s verbal communication and provides invaluable insights into their condition. Information gathered includes the patient’s chief complaint, pain levels (using a numerical scale or descriptive terms like mild, moderate, or severe), the duration and onset of symptoms, any aggravating or relieving factors, and the impact of the condition on their daily activities and functional limitations. It’s essential to record the patient’s perception of their progress, their goals for therapy, and any concerns or anxieties they may have. Accurate documentation of the patient’s subjective experience is paramount for tailoring effective treatment plans, establishing rapport, and tracking progress effectively. Examples found in various online PDF resources demonstrate how to concisely and accurately capture this essential information, ensuring compliance with documentation standards. The subjective portion provides context to the objective findings and guides the therapist’s assessment and treatment decisions. Detailed examples illustrate how to document patient-reported information without bias, focusing on factual accounts.
Objective (O)⁚ Therapist’s Observations
The objective section of a physical therapy SOAP note focuses on measurable and observable findings documented by the therapist. This section avoids subjective interpretations and relies on quantifiable data; Key elements include detailed observations of the patient’s posture, gait, range of motion (ROM) measurements using goniometry, muscle strength assessments using manual muscle testing (MMT), and functional assessments such as timed-up-and-go tests. Objective data also encompasses the therapist’s observations during specific treatment interventions. For example, the number of repetitions completed during an exercise, the patient’s response to manual therapy techniques, and any observed changes in pain or movement patterns should be recorded. The objective section may also document the use of physical modalities, such as ultrasound or electrical stimulation, including the parameters used. Online PDF examples illustrate how to effectively record objective data using standardized measurements and terminology. This ensures consistency and clarity, facilitating accurate progress tracking and communication with other healthcare professionals. Precise and detailed objective findings provide a clear picture of the patient’s physical status and response to treatment.
Assessment (A)⁚ Therapist’s Interpretation
The assessment section of a physical therapy SOAP note represents the therapist’s professional judgment based on the subjective and objective findings. This crucial section integrates the patient’s reported symptoms with the therapist’s observations to formulate a clinical impression. It involves analyzing the data collected to identify impairments, activity limitations, and participation restrictions according to the International Classification of Functioning, Disability, and Health (ICF) model. The assessment should clearly articulate the patient’s diagnosis and prognosis, considering the impact of their condition on their daily life and functional abilities; The therapist’s interpretation should connect the observed impairments to the patient’s functional limitations and participation restrictions. For example, decreased ROM might be linked to difficulty performing ADLs. Online PDF examples often demonstrate how to concisely and effectively summarize the assessment, highlighting key factors influencing the treatment plan. The assessment should justify the need for skilled physical therapy intervention, demonstrating medical necessity and guiding subsequent treatment decisions. Clear and concise assessment statements are paramount for effective communication and appropriate healthcare resource allocation.
Plan (P)⁚ Treatment Plan and Goals
The “Plan” section of a physical therapy SOAP note outlines the therapist’s proposed treatment strategy to address the patient’s identified impairments, activity limitations, and participation restrictions. This section should clearly articulate specific, measurable, achievable, relevant, and time-bound (SMART) goals. These goals should directly address the impairments and limitations identified in the assessment. The plan should detail the interventions to be used, including specific treatment modalities, exercises, and patient education. Frequency and duration of treatment should be specified, along with any assistive devices or home exercise programs (HEPs). Many online PDF examples illustrate how to structure this section effectively. The plan should demonstrate a clear progression towards the established goals and justify the use of skilled physical therapy services. For instance, the plan might outline a gradual increase in exercise intensity or a transition from manual therapy to self-management strategies. Careful documentation in this section ensures a cohesive and effective treatment plan, facilitating communication and ensuring appropriate care delivery. The plan should align with the patient’s individual needs and preferences, fostering a collaborative approach to rehabilitation.
Progress Notes and Discharge Summaries
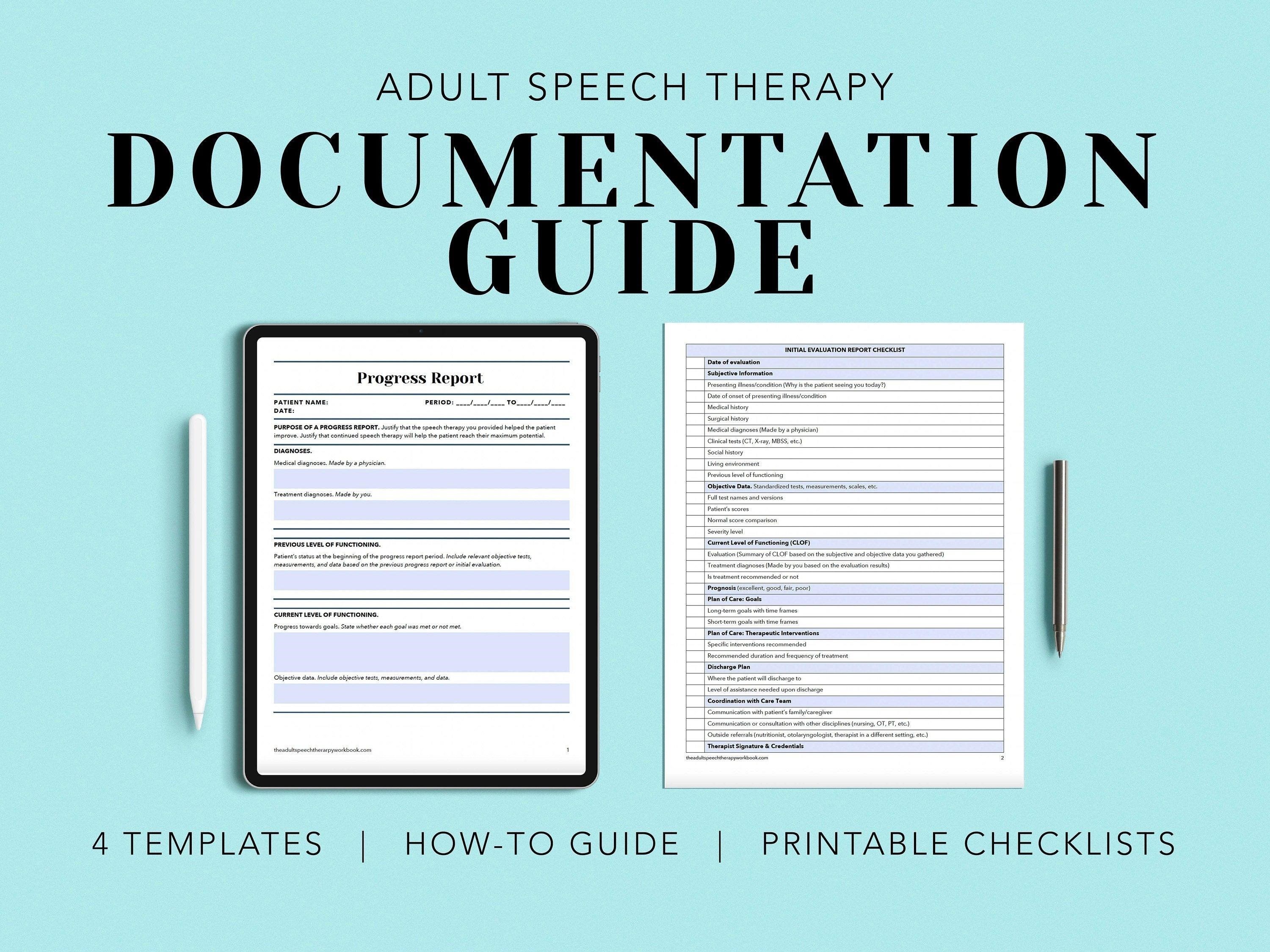
Progress notes, integral to ongoing physical therapy documentation, track a patient’s response to treatment over time. These notes, often found within readily available online PDF examples, detail changes in the patient’s subjective reports, objective measurements, and overall progress toward established goals. They document modifications to the treatment plan based on the patient’s response and any new information obtained. Progress notes demonstrate the necessity and skillfulness of ongoing physical therapy services, justifying continued care. Discharge summaries, on the other hand, provide a comprehensive overview of the patient’s entire course of therapy. They summarize the patient’s initial status, treatment provided, functional outcomes achieved, and any recommendations for continued care or home exercise programs. These summaries are crucial for communication with other healthcare providers and often serve as a vital record for future reference. Well-structured discharge summaries, which can also be found in various online PDF resources, clearly outline the patient’s progress and provide a concise, yet informative, conclusion to the episode of care. The quality of both progress notes and discharge summaries significantly impacts the overall effectiveness and comprehensiveness of physical therapy documentation.
Examples of Physical Therapy Documentation
Numerous online resources offer downloadable PDF examples of physical therapy documentation, showcasing various formats, including SOAP notes and progress reports. These examples illustrate effective documentation practices, offering valuable templates and guidance for practitioners.
Sample SOAP Note Templates
Many readily available online resources provide downloadable PDF files containing sample SOAP note templates for physical therapy documentation. These templates offer structured formats to guide the recording of patient information, facilitating efficient and comprehensive documentation. A well-structured SOAP note typically includes four sections⁚ Subjective (patient-reported information), Objective (therapist’s observations and measurements), Assessment (therapist’s professional judgment), and Plan (the outline of the treatment plan). These templates often include space for documenting specific details such as pain levels, range of motion, functional limitations, and treatment interventions. Using a standardized SOAP note format ensures consistency and clarity, making it easier for other healthcare professionals to understand and follow a patient’s progress. The use of these readily available templates helps streamline the documentation process, reducing the time spent on administrative tasks and allowing therapists to focus more on patient care. Free downloadable examples allow for practice before implementing in clinical settings. The availability of these resources emphasizes the importance of clear and concise documentation in physical therapy practice.
Specific Treatment Modality Documentation
Detailed documentation of specific treatment modalities is crucial for effective physical therapy. Many online resources provide examples in PDF format, illustrating how to accurately record the application of various techniques. These examples often include information on the type of modality used (e.g., ultrasound, electrical stimulation, manual therapy), the parameters of treatment (e.g., frequency, intensity, duration), the patient’s response to the treatment, and any observed adverse effects. Accurate documentation of these specifics is essential for demonstrating medical necessity and justifying the skilled services provided. The examples highlight the importance of clear and concise descriptions, ensuring that the documentation accurately reflects the interventions performed and their impact on the patient’s condition. These downloadable PDFs serve as valuable educational tools for physical therapists, promoting consistent and high-quality documentation practices. They often include examples of documentation for various conditions and patient populations, enhancing understanding and improving the overall quality of care provided.
Documentation for Different Settings (Outpatient, Inpatient)
Physical therapy documentation varies significantly depending on the care setting. Numerous online resources offer downloadable PDF examples showcasing documentation specifics for outpatient and inpatient settings. Outpatient documentation might focus on functional goals, home exercise programs, and patient progress toward discharge. In contrast, inpatient documentation emphasizes acute care needs, collaborative treatment with other disciplines, and daily progress notes reflecting the patient’s response to intensive interventions. These examples illustrate how the format, content, and level of detail differ based on the setting’s unique demands. The PDFs often include sample SOAP notes, progress notes, and discharge summaries tailored to each environment. Accessing these examples allows therapists to adapt their documentation to meet the specific requirements of different settings, ensuring clear communication and comprehensive records. The variations highlighted in these resources emphasize the importance of understanding the specific needs and requirements of each healthcare environment. This ensures that documentation remains compliant with regulatory standards and effectively communicates patient status and care provided.